MEASURE DESCRIPTION:
Percentage of patients, aged 18 years and older, undergoing selected surgical procedures that were managed with multimodal pain medicine.
NQS DOMAIN/MEANINGFUL MEASURE AREA:
Effective Clinical Care/Prevention and Treatment of Opioid and Substance Abuse Disorders
MEASURE TYPE:
Process
HIGH PRIORITY STATUS:
Yes
INSTRUCTIONS:
This measure is to be reported each time a patient undergoes a selected surgical procedure during the reporting period. It is anticipated that Merit-based Incentive Payment System (MIPS) eligible anesthesia providers and clinicians who provide denominator-eligible services will submit this measure.
MEASURE SUBMISSION TYPE:
Measure data may be submitted by individual MIPS eligible clinicians, groups, or third party intermediaries. The listed denominator criteria are used to identify the intended patient population. The numerator options included in this specification are used to submit the quality actions as allowed by the measure. The quality data codes listed do not need to be submitted by MIPS eligible clinicians, groups, or third party intermediaries that utilize this modality for submissions; however, these codes may be submitted for those third party intermediaries that utilize Medicare Part B claims data. For more information regarding Application Programming Interface (API), please refer to the Quality Payment Program (QPP) website.
DENOMINATOR:
Patients, aged 18 years and older, who undergo selected surgical procedures
Denominator Note: Selected surgical procedures include both elective and urgent open and laparoscopic intra-abdominal, spinal, pelvic, thoracic, breast, joint, head, neck, orthopedic and fracture repair surgeries.
-
Denominator Criteria (Eligible Cases):
Patients aged 18 years and older on date of encounter
AND
Patient procedures during reporting period (CPT):
00102, 00120, 00160, 00162, 00172, 00174, 00190, 00222, 00300, 00320, 00402, 00404, 00406, 00450, 00470, 00472, 00500, 00528, 00529, 00539, 00540, 00541, 00542, 00546, 00548, 00600, 00620, 00625, 00626, 00630, 00670, 00700, 00730, 00750, 00752, 00754, 00756, 00770, 00790, 00792, 00794, 00797, 00800, 00820, 00830, 00832, 00840, 00844, 00846, 00848, 00860, 00862, 00864, 00865, 00866, 00870, 00872, 00873, 00880, 00902, 00906, 00910, 00912, 00914, 00916, 00918, 00920, 00940, 00942, 00948, 01120, 01160, 01170, 01173, 01210, 01214, 01215, 01220, 01230, 01360, 01392, 01400, 01402, 01480, 01482, 01484, 01486, 01630, 01634, 01636, 01638, 01740, 01742, 01744, 01760, 01830, 01832, 01961
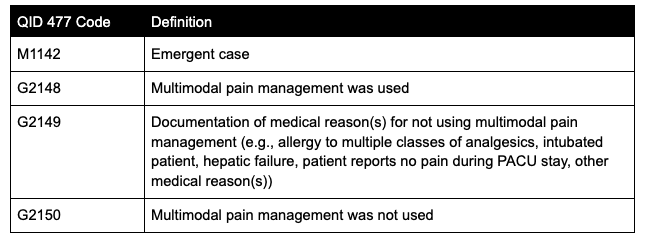
AND NOT - Denominator Exclusion: Emergent cases: M1142
NUMERATOR:
Patients for whom multimodal pain management is administered in the perioperative period from 6 hours prior to anesthesia start time until discharged from the post-anesthesia care unit
Numerator Definition: Multimodal pain management is defined as the use of two or more drugs and/or interventions, NOT including systemic opioids, that act by different mechanisms for providing analgesia. These drugs and/or interventions can be administered via the same route or by different routes. Opioids may be administered for pain relief when indicated but will not count toward this measure.
Numerator Note: Documentation of qualifying medications or interventions provided from six hours prior to anesthesia start time through post-anesthesia care unit discharge count toward meeting the numerator.-
Numerator Options:
Performance Met: Multimodal pain management was used (G2148)
OR
Performance Not Met: Multimodal pain management was not used (G2150)
OR
Denominator Exception: Documentation of medical reason(s) for not using multimodal pain management (e.g., allergy to multiple classes of analgesics, intubated patient, hepatic failure, patient reports no pain during PACU stay, other medical reason(s)) (G2149)
RELEVANT FIELDS:
- Date of procedure
- Date of birth
- ASA CPT code
- Elective case
- Multimodal pain management used
RATIONALE:
Besides providing anesthesia care in the operating room, anesthesiologists are dedicated to providing the best perioperative pain management in order to improve patients’ function and facilitate rehabilitation after surgery. In the past, pain management was limited to the use of opioids (also called narcotics). Opioids provide analgesia primarily through a unitary mechanism, and just adding more opioids does not usually lead to better pain control or improve outcomes. In fact, opioids are responsible for a host of side effects that can be a threat to life, and increasing rates of complications after surgery can be attributed to the overuse and abuse of opioids. In 2012, the American Society of Anesthesiologists (ASA) published its guidelines for acute pain management in the perioperative setting (1), and ASA along with the American Society of Regional Anesthesia and Pain Medicine (ASRA) and American Pain Society collaborated on the 2016 clinical practice guidelines for the management of postoperative pain (2). These documents endorse the routine use of “multimodal analgesia” which means employing multiple classes of pain medications or therapies, working with different mechanisms of action, in the treatment of acute pain instead of relying on opioids alone.
While opioids may continue to be important pain medications, they must be combined with other classes of medications known to prevent and help relieve postoperative pain unless contraindicated. The list includes but is not limited to:
-
Non-steroidal anti-inflammatory drugs (NSAIDs): Examples include ibuprofen, diclofenac, ketorolac, celecoxib, nabumetone. NSAIDs act on the prostaglandin system peripherally and work to decrease inflammation.
-
NMDA antagonists: When administered in low dose, ketamine, magnesium, and other NMDA antagonists act on the N-methyl-D-aspartate receptors in the central nerve system to decrease acute pain and hyperalgesia.
-
Acetaminophen: Acetaminophen acts on central prostaglandin synthesis and provides pain relief through multiple mechanisms.
-
Gabapentinoids: Examples include gabapentin and pregabalin. These medications are membrane stabilizers that essentially decrease nerve firing.
-
Regional block: The ASA and ASRA also strongly recommend the use of target-specific local anesthetic applications in the form of regional analgesic techniques as part of the multimodal analgesic protocol whenever indicated.
-
Steroids: Dexamathasone during surgery has been shown to decrease pain and opioid requirements.
-
Local anesthetics: Injection of local anesthetic in or around the surgical site by the surgeon is an example. Systemic lidocaine administered intravenously represents an alternative to regional analgesic techniques.
REPORTING CODES: