MEASURE DESCRIPTION:
Percentage of patients, aged 18 years and older, undergoing elective total joint arthroplasty who were screened for anemia preoperatively AND, if positive, have documentation that one or more of the following management strategies were used prior to PACU discharge.
Management strategies include one or more of the following:
- Cell salvage techniques employed intraoperatively
- Intraoperative antifibrinolytic therapy or tourniquet, if not contraindicated
- Preoperative iron supplementation, epoetin alpha
- Use of evidence-based preoperative anemia management algorithm supplemented with laboratory testing and/or multidisciplinary consult
NQS DOMAIN/MEANINGFUL MEASURES AREA:
Patient Safety/Preventable Healthcare Harm
MEASURE TYPE:
Process
HIGH PRIORITY STATUS:
Yes
INVERSE MEASURE:
No
RISK ADJUSTED:
No
INSTRUCTIONS:
This measure is to be reported each time a patient undergoes an elective total joint arthroplasty procedure during the reporting period. It is anticipated that qualified anesthesia providers and eligible clinicians who provide denominator- eligible services will submit this measure.
Measure Reporting via the Qualified Clinical Data Registry
Patient demographics and CPT codes are used to identify patients who are included in the measure denominator. G-codes and Registry Codes are used to capture the numerator.
DENOMINATOR:
Patients, aged 18 years and older, undergoing elective total joint arthroplasty.
Denominator Note: For the purpose of this measure, total joint arthroplasty includes arthroplasty of the knee, hip, and shoulder.
-
Denominator Criteria (Eligible Cases):
All patients, aged 18 years and older
AND
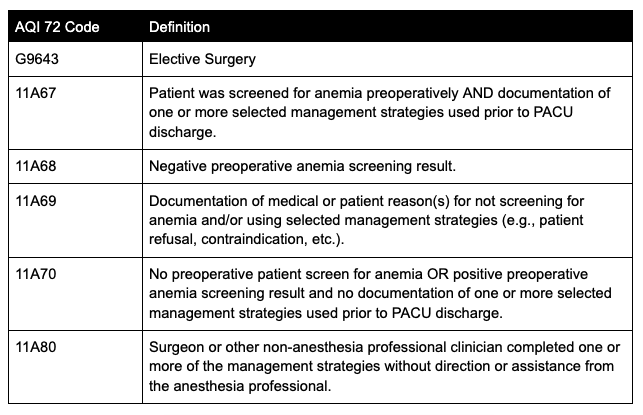
Elective Surgery: G9643
AND
Patient encounter during the reporting period (CPT):
01214, 01215, 01402, 01638
- Denominator Exclusions:
Surgeon or other non-anesthesia professional clinician completed one or more of the management strategies without direction or assistance from the anesthesia professional. (11A80)
NUMERATOR:
Patients who were screened for anemia preoperatively AND, if positive, have documentation that one or more of the following management strategies were used prior to PACU discharge.
Management strategies include one or more of the following:
- Cell salvage techniques employed intraoperatively
- Intraoperative antifibrinolytic therapy or tourniquet, if not contraindicated
- Preoperative iron supplementation, epoetin alpha
- Use of evidence-based preoperative anemia management algorithm supplemented with laboratory testing and/or multidisciplinary consult
Numerator Definition: For the purpose of this measure, a positive preoperative anemia screening result is defined as a Hgb value <13 gm/dL all adults, regardless of gender.
Numerator note: Preoperative screening for anemia could include any of the following tests: complete blood count (CBC), arterial blood gas (ABG), venous blood gas (VBG), or other point of care hemoglobin/hematocrit test within 90 days and until one day prior to the surgical procedure.- Numerator Options:
Performance Met: Patient was screened for anemia preoperatively AND documentation of one or more selected management strategies used prior to PACU discharge. (11A67)
OR
Performance Not Met: No preoperative patient screen for anemia OR positive preoperative anemia screening result and no documentation of one or more selected management strategies used prior to PACU discharge. (11A70)
OR
Denominator Exception: Negative preoperative anemia screening result. (11A68)
OR
Denominator Exception: Documentation of medical or patient reason(s) for not screening for anemia and/or using selected management strategies (e.g., patient refusal, contraindication, etc.). (11A69)
RELEVANT FIELDS:
- Date of service
- Date of birth
- ASA CPT code
- Anemia screen
- Anemia present
RATIONALE:
Anemia is a common complication of many chronic illnesses that interferes with iron absorption. It has been estimated that at least one-third of patients undergoing non-emergent surgical procedures have potentially treatable anemia. Preoperative anemia is associated with increased need for perioperative blood transfusion as well as significant perioperative morbidity and mortality. Appropriate preoperative anemia management can reduce the risk
of perioperative blood transfusion, help identify co-morbidities, and improve perioperative outcomes by improving patients’ readiness for surgery. The 2015 American Society of Anesthesiologists Guideline on Perioperative Blood Management indicate “TEG and ROTEM-guided algorithms are shown to be effective in reducing blood transfusion requirements.” Additionally, studies have found that preoperative anemia has been associated with postoperative joint infections. The preoperative screening for anemia would reduce the number of post-operative joint infections.” More resources can be found at the American Association of Blood Banks.
The purpose of this measure is to drive quality changes within perioperative anemia management. Testing algorithms may not be available in all practices. Those that do not have testing algorithms should use a different strategy to fulfill requirements of this measure.
REPORTING CODES: