MEASURE DESCRIPTION:
Percentage of patients aged 18 years or older, who undergo an elective procedure lasting 30 minutes or longer requiring inhalational general anesthesia who during the maintenance phase of the anesthetic have a total fresh gas flow less than or equal to 1 L/min (less than or equal to 2 L/min for Sevoflurane).
NQS DOMAIN/MEANINGFUL MEASURES AREA:
Efficient Use of Healthcare Resources/Clinical Process/Effectiveness
MEASURE TYPE:
Process
HIGH PRIORITY STATUS:
Yes
INVERSE MEASURE:
No
INSTRUCTIONS:
This measure is to be reported each time a patient undergoes an elective procedure in which inhalational general anesthesia is used. It is anticipated that qualified anesthesia providers and eligible clinicians who provide denominator-eligible services will submit this measure.
Measure Reporting via the Qualified Clinical Data Registry
Patient demographics and CPT codes are used to identify patients who are included in the measure denominator. G-codes and Registry Codes are used to capture the numerator.
DENOMINATOR:
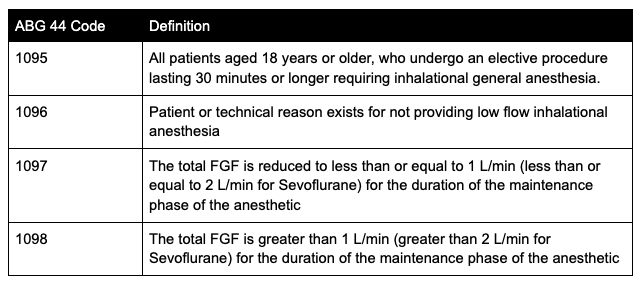
All patients aged 18 years or older, who undergo an elective procedure lasting 30 minutes or longer requiring inhalational general anesthesia. (1095)
-
Denominator Criteria (Eligible Cases):
Patients aged 18 years and older
AND
Elective procedure
AND
Patient who receives inhalational general anesthesia
AND
Procedure lasts 30 minutes or longer
AND
Patient encounter during the reporting period (CPT)
00100, 00102, 00103, 00104, 00120, 00124, 00126, 00140, 00142, 00144, 00145, 00147, 00148, 00160, 00162, 00164, 00170, 00172, 00174, 00176, 00190, 00192, 00210, 00211, 00212, 00214, 00215, 00216, 00218, 00220, 00222, 00300, 00320, 00322, 00350, 00352, 00400, 00402, 00404, 00406, 00410, 00450, 00454, 00470, 00472, 00474, 00500, 00520, 00522, 00524, 00528, 00529, 00530, 00532, 00534, 00537, 00539, 00540, 00541, 00542, 00546, 00548, 00550, 00560, 00566, 00580, 00600, 00604, 00620, 00625, 00626, 00630, 00632, 00635, 00640, 00670, 00700, 00702, 00730, 00731, 00732, 00750, 00752, 00754, 00756, 00770, 00790, 00792, 00794, 00796, 00797, 00800, 00802, 00811, 00812, 00813, 00820, 00830, 00832, 00840, 00842, 00844, 00846, 00848, 00851, 00860, 00862, 00864, 00865, 00866, 00868, 00870, 00872, 00873, 00880, 00882, 00902, 00904, 00906, 00908, 00910, 00912, 00914, 00916, 00918, 00920, 00921, 00922, 00924, 00926, 00928, 00930, 00932, 00934, 00936, 00938, 00940, 00942, 00944, 00948, 00950, 00952, 01112, 01120, 01130, 01140, 01150, 01160, 01170, 01173, 01200, 01202, 01210, 01212, 01214, 01215, 01220, 01230, 01232, 01234, 01250, 01260, 01270, 01272, 01274, 01320, 01340, 01360, 01380, 01382, 01390, 01392, 01400, 01402, 01404, 01420, 01430, 01432, 01440, 01442, 01444, 01462, 01464, 01470, 01472, 01474, 01480, 01482, 01484, 01486, 01490, 01500, 01502, 01520, 01522, 01610, 01620, 01622, 01630, 01634, 01636, 01638, 01650, 01652, 01654, 01656, 01670, 01680, 01710, 01712, 01714, 01716, 01730, 01732, 01740,01742, 01744, 01756, 01758, 01760, 01770, 01772, 01780, 01782, 01810, 01820, 01829, 01830, 01832, 01840, 01842, 01844, 01850, 01852, 01860, 01924, 01925, 01926, 01930, 01931, 01932, 01933, 01935, 01936, 01951, 01952, 01961, 01962, 01963, 01965, 01966
-
Denominator Exceptions:
Patient or technical reason exists for not providing low flow inhalational anesthesia (e.g., flow meter not capable of generating low flows, patient hypermetabolic, lack of CO2 absorbents without KOH and low concentrations of NaOH, etc.) (1096)
NUMERATOR:
Patients who undergo an elective procedure lasting 30 minutes or longer requiring inhalational general anesthesia who during the maintenance phase of the anesthetic have a total fresh gas flow less than or equal to1 L/min (less than or equal to 2 L/min for Sevoflurane).
Numerator Note: Inhalational general anesthesia is defined as the use of at least one inhalational anesthetic gas (e.g., halothane, isoflurane, desflurane, sevoflurane, nitrous oxide) as the primary mode of anesthesia for the procedure.
Numerator Note: The maintenance phase of the inhalational anesthetic is defined as the portion of the case in which Stage III surgical anesthesia (e.g., unconsciousness, amnesia, immobility, unresponsive to surgical stimulation) is achieved at a safe anesthetic depth while also maintaining respiratory and hemodynamic stability. This occurs between the induction and emergence phases of the case.1
Numerator Note: Fresh gas flow (FGF) is defined as the combined admixture of medical gases such as air, oxygen, or nitrous oxide as well as volatile anesthetics as set by the anesthesia provider.
-
Numerator Options:
Performance Met: The total FGF is reduced to less than or equal to 1 L/min (less than or equal to 2 L/min for Sevoflurane) for the duration of the maintenance phase of the anesthetic (1097).
ORPerformance Not Met: The total FGF is greater than 1 L/min (greater than 2 L/min for Sevoflurane) for the duration of the maintenance phase of the anesthetic (1098).
RELEVANT FIELDS:
-
ASA CPT code
-
Inhalational agent used
-
Anesthesia start
-
Anesthesia end
-
Emergency status
-
Patient age
RATIONALE:
Managing Fresh Gas Flow to Reduce Environmental Contamination
Introduction
When using a circle anesthesia system, any anesthetic gases and vapors that enter the scavenging system will flow through the hospital vacuum system and ultimately be vented outside the hospital to the atmosphere. The total fresh gas flow determines the amount of gas entering the scavenging system per minute. Whenever fresh gas flow exceeds the patient‘s requirement, gases and vapors will enter the scavenging system and ultimately contaminate the atmosphere. By choosing the minimal total fresh gas flow, the environmental impact of anesthetic vapors and gases can be minimized. Although the environmental impact of a single case may be minimal, every practitioner can make a significant difference over the thousands of procedures during their career by practicing careful fresh gas flow management for each case. There are three strategies to minimize fresh gas flow and environmental contamination. To implement these strategies, it is important to understand how to utilize anesthetic agent and oxygen concentration monitors to safely deliver the minimum fresh gas flow.
Strategy #1: Minimize Fresh Gas Flow During Maintenance
With this background, the first strategy to reduce the environmental impact of anesthetic vapors is to minimize the fresh gas flow during the maintenance phase of the case. As an example of a low, or minimal, flow anesthetic technique, consider a case of a 70 kg male requiring general anesthesia. Following intravenous induction, isoflurane was administered using oxygen and air at 2 L/min each for a total fresh gas flow of 4 L/min. Once the exhaled concentration of isoflurane is close to the inspired concentration, uptake from the lungs has slowed and the fresh gas flow can be reduced. Assuming oxygen consumption to be about 350 mL/min, the oxygen flow can be set to 350 mL/min. The air flowmeter can be set at 500 mL/min which would deliver an additional 105 mL/min of oxygen and the total fresh gas flow will be less than 1 L/min. If nitrous oxide is used, the oxygen flowmeter should be set to 500 mL/min at a minimum and nitrous oxide at 500 mL/min.
Managing this technique requires that the inspired oxygen concentration be monitored. If oxygen consumption exceeds the total oxygen delivered, the inspired oxygen concentration will diminish over time, which will be an indication that oxygen flow needs to be increased. There is still some environmental contamination with this technique, since the total fresh gas flow exceeds what is consumed, but it is easier to manage than a true “closed circuit” technique. Unless the patient has a large oxygen consumption (e.g., trauma, pregnancy) it should be possible during the maintenance phase of anesthesia to limit the fresh gas flow to a maximum of 1 L/minute. For smaller patients with even lower oxygen consumption requirements, the maintenance fresh gas flow can be reduced even further with the same caveat of monitoring inspired oxygen concentration.
Greening the Operating Room and Perioperative Arena: Environmental Sustainability for Anesthesia Practice. Task Force on Environmental Sustainability Committee on Equipment and Facilities, American Society of Anesthesiologists (ASA).
https://www.asahq.org/about-asa/governance-and-committees/asa-committees/committee-on-equipment-and- facilities/environmental-sustainability/greening-the-operating-room#3gas
Described in 1952 by Foldes, the technique of reducing the fresh gas flow during an anesthetic to a level < 1 L/min is both safe and effective.2 Additionally, there are benefits to both the patient, cost savings to the facility and benefits to the environment.3
-
The inhalational anesthetic agents sevoflurane isoflurane and desflurane have global warming potentials 2-3 orders of magnitude higher than CO2.3
-
Nitrous oxide contributes significantly to global warming and ozone depletion.3
-
5% of the carbon footprint (CO2e) of the British National Health System is attributable to exhaled anesthetic agents.3
-
Reducing the environmental impact of anesthesia, can be achieved through behavior change.3
-
The chemical properties and global warming impacts of these gases vary, with atmospheric lifetimes of 1−5 years for sevoflurane, 3−6 years for isoflurane, 9−21 years for desflurane, and 114 years for N2O.4
-
The conservation of heat and moisture within the breathing system is an added benefit of low flow anesthesia to the patient especially when humidifier connection filters are not used.
-
Low flow anesthesia can result in cost savings even when the increased cost of CO2 absorber is factored in,
-
especially with regards to usage of Sevoflurane and Desflurane.5
-
The simulated low flow anesthesia of 1 L/min FGF across all agents predicted a 48% reduction in costs of volatile anesthetics at a tertiary hospital.6
REPORTING CODES: